
PMHNP Market Pulse
The PMHNP Job Market Newsletter · Mar 10, 2026
A patient says their anxiety “came out of nowhere,” but their sleep log lines up perfectly with late-night scrolling and doom-heavy content. Another is stable on meds—until a new short-form trend starts reinforcing compulsions, body checking, or paranoid interpretations.
We’re seeing social media show up as a real clinical variable: exposure, reinforcement, sleep disruption, and identity stress—often in the same visit.
We’re seeing social media show up as a real clinical variable: exposure, reinforcement, sleep disruption, and identity stress—often in the same visit.
The Quick Take
Treat the feed like an exposure source.
We’re hearing more “algorithm-shaped” symptom patterns: panic spikes after specific creators, self-harm content that slips through, OCD reassurance loops, and manic spending triggered by shopping streams. A practical frame is: what content, how often, and what happens after—mood, sleep, urges, and behavior.
Differential: education vs. escalation.
“Mental health TikTok” can normalize help-seeking, but it can also push self-diagnosis, black-and-white thinking, and medication fear. When a patient brings a label, we can validate the distress while clarifying: duration, impairment, rule-outs, and functional change—not just symptom lists.
Document the digital context (briefly, consistently).
A tight note helps continuity: baseline use, late-night use, triggering themes, and any safety-relevant exposure (self-harm content, harassment, stalking, sextortion). It’s often enough to add a single line: “Symptoms correlate with social media exposure and sleep disruption; plan includes boundaries + skills.”
Build a “digital hygiene” plan that patients can follow.
Vague advice (“scroll less”) rarely sticks. Better: time windows, sleep protection, content rules, and replacement behaviors. We’re also seeing stronger adherence when patients choose one measurable change for 7 days and track mood/sleep alongside it.
One Number That Matters
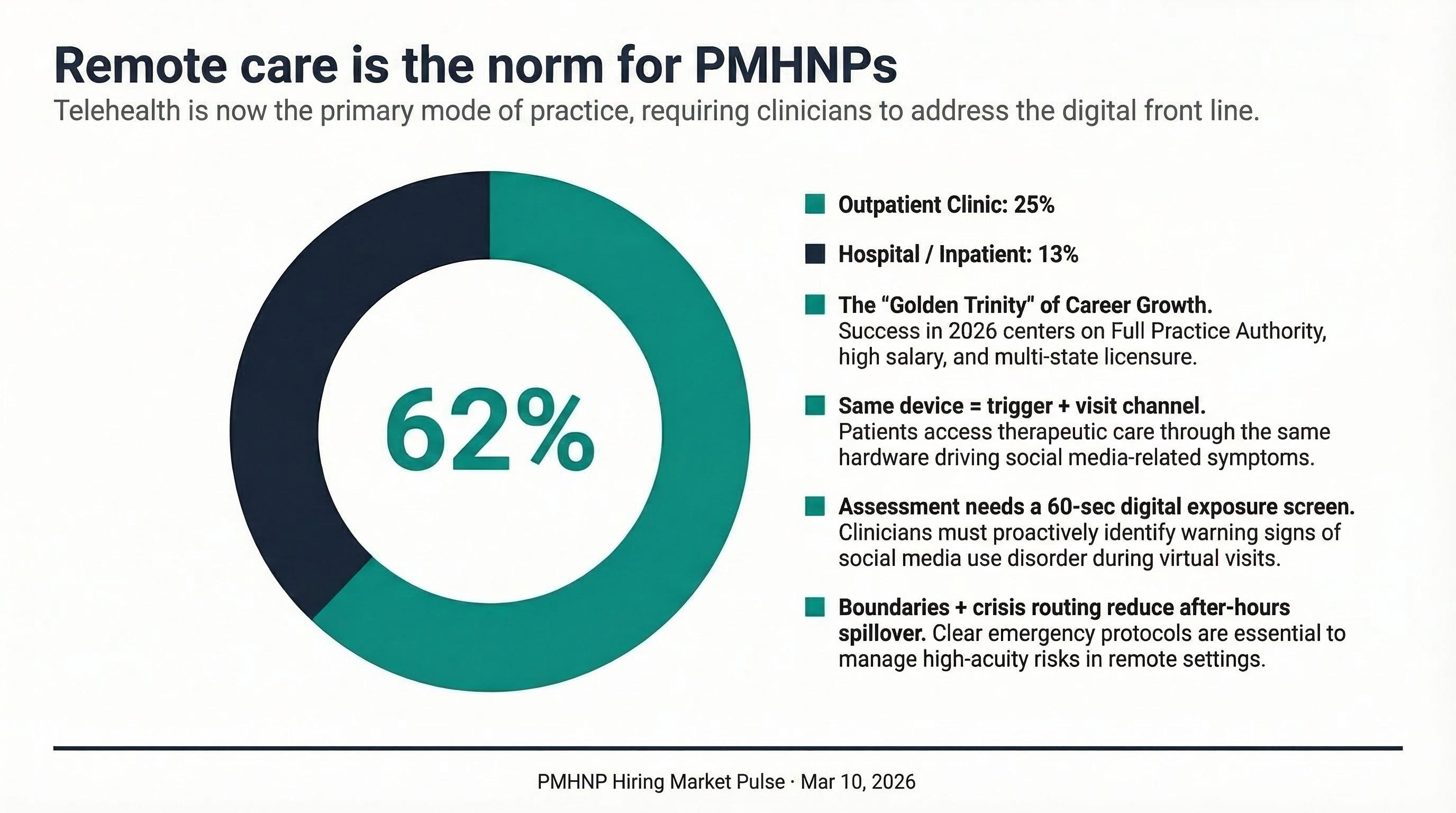
62% of PMHNP roles are remote-eligible. That matters because the same devices driving symptoms are also the care channel—so assessment, boundary-setting, and safety planning have to work in a telehealth workflow.
What To Do With This
Add a 60-second “digital exposure” screen to intakes and follow-ups: bedtime scrolling, triggering themes, DMs/harassment, and symptom-after-scroll. Then prescribe one concrete boundary (example: no algorithm feeds after 9 pm + phone out of bedroom) and pair it with a replacement (music, brief walk, grounding, or a scheduled check-in with supports).
If you’re job searching, ask employers how they handle after-hours messaging, crisis routing, and documentation expectations in remote care—those policies determine whether social-media-driven crises become your unpaid inbox.
If you’re job searching, ask employers how they handle after-hours messaging, crisis routing, and documentation expectations in remote care—those policies determine whether social-media-driven crises become your unpaid inbox.
🔔 Don't miss your next role.
Get new PMHNP roles that match your preferences sent to your inbox—so you can look between patients, not after a 12-hour day.
— The PMHNP Hiring Team
P.S. If you’re seeing a new “trend” driving symptoms, reply with the pattern (no patient details). We’ll track what’s showing up across settings.
Know a PMHNP who'd find this useful?
Forward this email or share: newsletter.pmhnphiring.com